Nine Systems. Zero Shared Identity. One Patient.
The identity problem at the heart of specialty care — and Technology enabled HUBs are building to finally fix it.
3/11/20267 min read

I was mapping the patient journey for an oncology pharma client back in 2018 — one of those engagements — where you go in thinking you understand the complexity, and leave humbled by how difficult the therapy is for the patient.
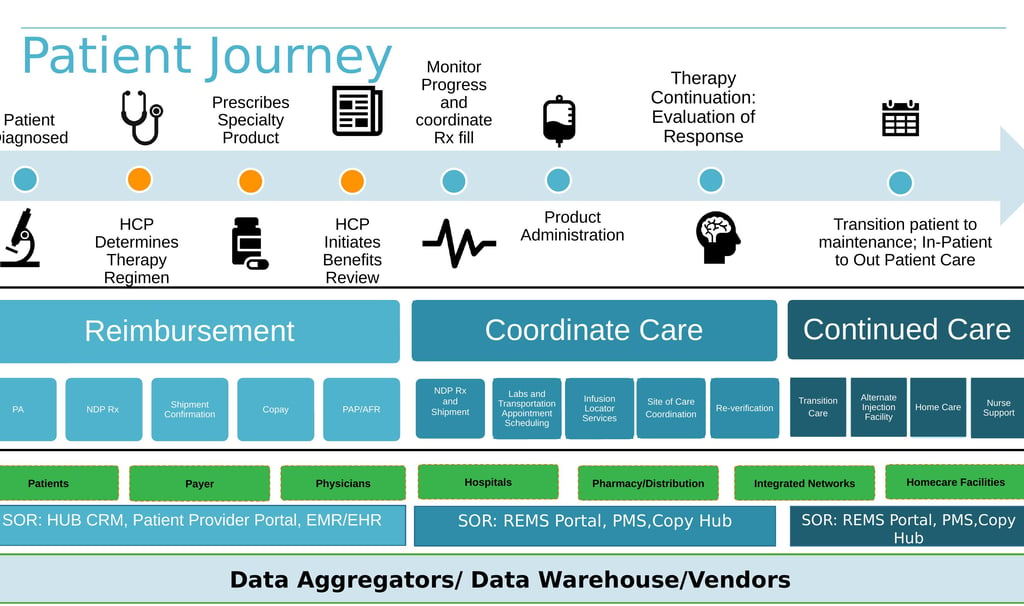
The map covered everything: from diagnosis and specialty prescribing through benefits verification, prior authorization, copay enrollment, patient assistance programs, NDP Rx, shipment confirmation, lab scheduling, infusion locator services, site-of-care coordination, re-verification, transition care, and nurse support.
Across seven distinct stakeholder groups: HCPs, patients, payers, physicians, hospitals, specialty pharmacies, integrated networks, and home care facilities.
Across five separate systems of record: the PBM and payer (connected via EDI 270/271/278), the EHR, the REMS portal, the specialty Rx system, the copay hub, and the HUB CRM.
Patient Journey Map — Oncology Pharma Client, Artha Consulting Lab / Soladis AI, 2018
Every system in that map sees a different version of the same patient. The payer has a member ID. The EHR has an MRN. The specialty pharmacy has a dispensing record. The HUB CRM has a case number. The copay hub has an enrollment ID.
None of them are automatically connected. None of them sync in real time.
And the problem doesn’t stop when treatment begins — it compounds. An oncology patient doesn’t stay in one place. They change insurers mid-therapy. They move between infusion centers, hospitals, and home care. They transition between treating physicians and healthcare networks. With each move, the data gap widens.
The Data Gap
Stakeholders providing care lose sight of the patient entirely at each transition. The specialty pharmacy dispatches a refill without knowing the patient’s benefits just changed payers. The HUB coordinator takes a call with yesterday’s prior auth status on screen. The Field Reimbursement Manager reports adherence data to the manufacturer — but has no visibility into the gaps created by the last network transition. And the patient, who just finished a chemotherapy cycle, calls the HUB helpline and spends fifteen minutes re-explaining their own case to a coordinator who should already have it.
That’s not a workflow problem. That’s not a change management problem. That’s an architecture problem.
What fragmented identity actually costs
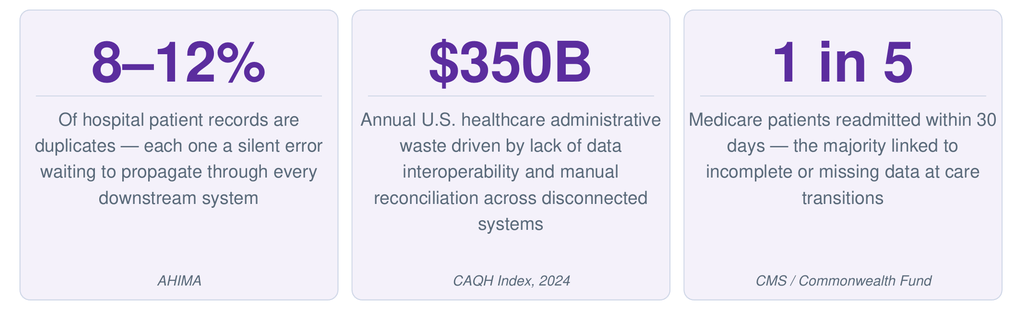
The cost of having no shared patient identity isn’t abstract — it shows up directly in the numbers.
Think about what a duplicate record actually means in practice. A patient whose identity exists differently in the PBM, the EHR, and the HUB CRM isn’t just a data quality problem — they’re a patient whose prior auth history, benefit status, and clinical notes are each living in a different silo. When something goes wrong, no single person can see the full picture.
The readmission number tells the same story from the clinical side. When a patient transitions from inpatient oncology to outpatient infusion to home care — and each setting has a different patient record — the handoff fails silently. No alert. No error message. Just a gap in the data that someone eventually discovers too late.
Industry analysis suggests specialty care teams routinely manage nine or more separate digital applications per complex patient. Each application has its own patient identifier, its own update cadence, and its own reconciliation burden. The AI operating across those systems doesn’t see a patient — it sees nine partial records that may or may not belong to the same person.
This is the version of AI failure no one talks about. Not the AI making the wrong recommendation. The AI never being given the data it needed to make any recommendation at all.
What the industry is finally building
The good news: the infrastructure to solve this is being built right now. And the bets being placed are significant.
Health100 — CVS Health & Google Cloud (March 2026)
CVS Health and Google Cloud announced Health100, a new subsidiary and consumer health platform built to be “an always-on personal health partner” that works regardless of which pharmacy, payer, PBM, provider, or digital health solution a consumer uses. The stated goal: support 100% of a consumer’s health, across all parts of the healthcare system. Technical foundation: Google’s Gemini models, Cloud Healthcare API, BigQuery, and “robust healthcare interoperability infrastructure to fully connect the healthcare partner ecosystem.” That’s the right model — a platform that doesn’t own the patient data, but connects it.
Innovaccer Gravity — Healthcare Intelligence Platform (2025)
Innovaccer launched Gravity, a healthcare intelligence platform that connects 400+ data sources into a single source of truth and resolves patient, provider, and organizational identity across the enterprise. In November 2025, Gravity was deployed specifically for specialty pharmacy through a partnership with Longitude Rx — unifying fragmented data across EMRs, payers, and pharmacies in real time, automating reimbursement workflows, and enabling real-time specialty order surfacing for health systems.
Salesforce Life Sciences Cloud — Agentic AI for Patient Services (2026)
Salesforce has evolved its HUB tooling toward pre-built AI agents for prior authorization, patient enrollment, adherence monitoring, and benefit verification — agents that work across the fragmented ecosystem rather than within any single system. More than 70 life sciences companies — including Pfizer, Takeda, and Boehringer Ingelheim — have adopted Salesforce’s Health Cloud or Life Sciences Cloud platform.
These aren’t small experiments. These are structural infrastructure bets that the industry is placing on unified patient intelligence as the next operating layer for healthcare.
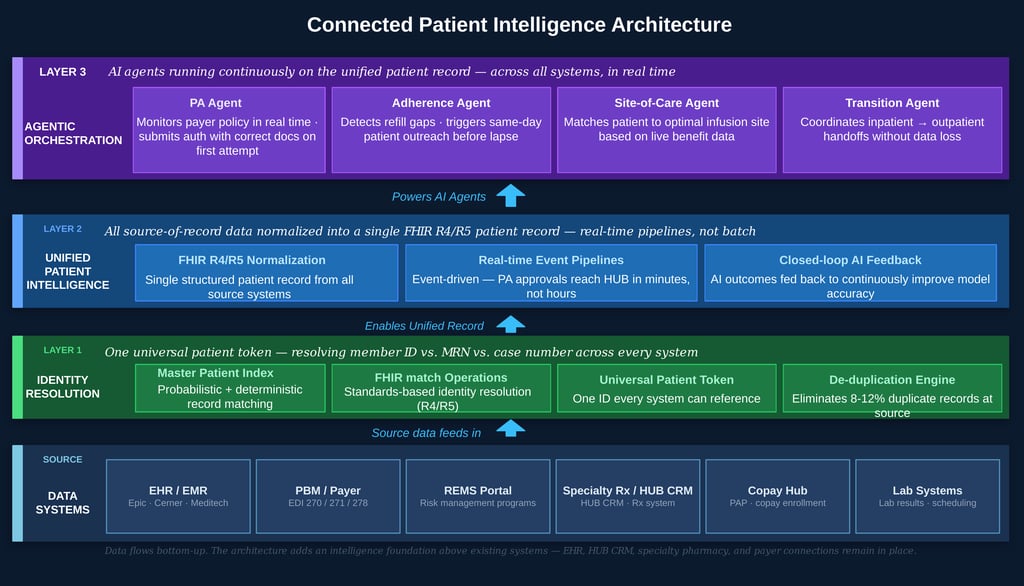
A new paradigm: The Connected Patient Intelligence Architecture
Here is the framework I want to leave you with. It’s the architecture that makes everything else in this series possible.
The old model treats each system as a point solution: the EHR is for clinical records, the HUB CRM is for case management, the PBM system is for claims. They hand off sequentially. Patient data sits in each silo and rarely travels.
Here is where most adoption conversations break down: the assumption that fixing the foundation requires throwing away everything built on top of it. That assumption is wrong.
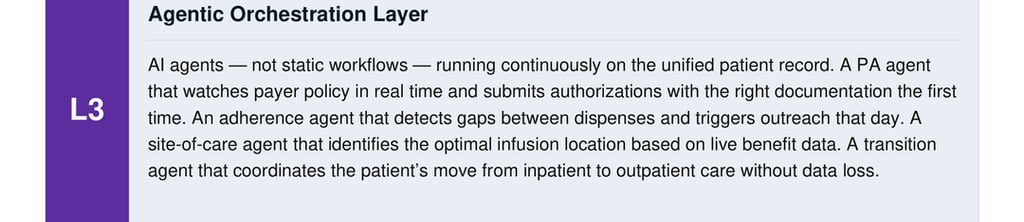
The new model adds three layers that sit above and across your existing systems — without replacing your EHR, your HUB CRM, your specialty pharmacy integrations, or your payer connections. You are not starting over. You are adding a foundation underneath what you already have.
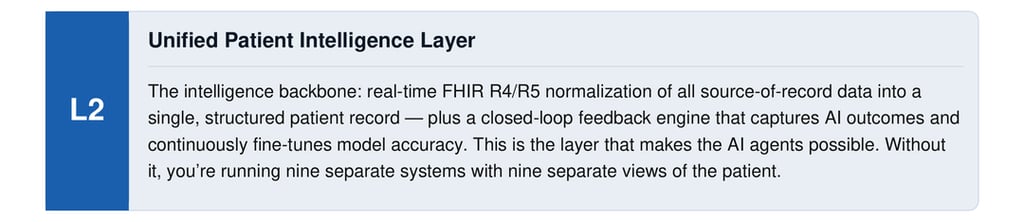
L2
Figure 1: Connected Patient Intelligence Architecture for HUB Operations
The critical insight is that the HUB isn’t bypassed by this architecture — it becomes the central node. When patient identity is resolved, when data is unified in real time, when AI agents can orchestrate across all systems, the HUB becomes the intelligence layer for the entire patient access journey.
Not a service vendor with a CRM. An AI-powered coordination platform with a unified, real-time view of every patient, every payer, and every transition point.
Three things HUBs can start building now
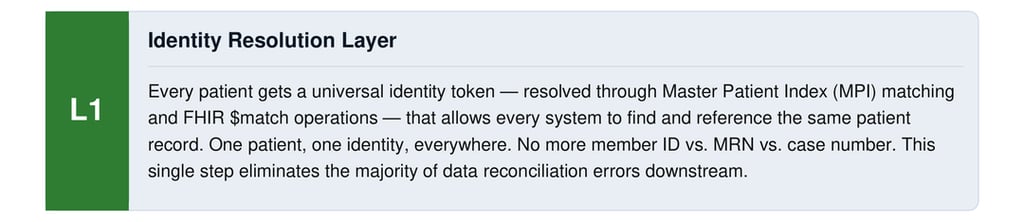
1. Resolve patient identity
Deploy a Master Patient Index or use FHIR $match to create a unified patient identifier that works across your EHR interface, your payer connections, and your HUB CRM. This single step eliminates the majority of downstream data reconciliation errors. You don’t need to rebuild your entire data infrastructure to do this — you need to add one identity resolution layer on top of what you have.
2. Build real-time data pipelines
Move away from nightly batch extracts toward event-driven FHIR feeds. When a payer approves a PA, your HUB should know within minutes, not hours. When a patient misses a refill, your adherence system should trigger outreach that day — not at the next weekly case review. The delay between event and action is where patients fall through the cracks.
3. Start with one agentic workflow
Don’t try to automate everything at once. Pick your highest-friction workflow — most likely prior authorization — and deploy an AI agent that handles the end-to-end process for the top five payers you interact with most. Measure first-pass approval rate, average turnaround time, and staff hours per approval. Then expand. Proving ROI on one workflow makes the next investment easier.
The window is open — for now
The RAND finding that opened this series still holds: 80% of AI projects fail, and data quality is the #1 root cause.
The difference now is that the infrastructure to solve the data problem exists. Health100, Innovaccer Gravity, Salesforce Life Sciences Cloud — these platforms are proof that unified patient intelligence is buildable. FHIR R4/R5 and TEFCA have created the standards backbone. Agentic AI has created the execution layer.
The HUBs that adopt this architecture in the next 18 months won’t just improve their operations. They will become genuinely irreplaceable partners in the patient access journey — because they’ll hold the only complete, real-time view of the patient across every system and every stakeholder.
The ones that don’t will be competing on price with every other manual service provider — doing the same fragmented, paper-trail coordination they did in 2018.
Disconnected care isn’t inevitable. It’s an architecture choice. And it’s one that the industry is finally, concretely, beginning to unmake.
About this series
If you’re working on any of these layers — identity resolution, FHIR integration, agentic PA, or HUB platform architecture — drop a comment. I’d like to know where HUBs actually are in this journey.
Ankur Jain, J.D., MBA
Sources: AHIMA Duplicate Patient Record Report; CAQH Index 2024; CMS 30-Day Readmission Data; Commonwealth Fund Care Transitions Research; Innovaccer Gravity Platform (businesswire.com, Nov 2025); CVS Health & Google Cloud Health100 announcement (prnewswire.com, Mar 2026); Salesforce Life Sciences Cloud; RAND Corporation AI Project Failure Research.