One HUB Problem Sat Unsolved for 8 Years. Here's What Finally Cracked It.
Eight years of the same specialty pharma HUB problem — from TBD placeholders in 2018 to AI in production in 2026. Here's what finally cracked it.
Ankur Jain, Esq. (J.D., MBA, POPM, SAFe Agilist)
3/4/20265 min read

I've Been Solving the Same HUB Problem Since 2018.
Here's What Finally Changed.
15+ years in specialty pharma access and adherence. Across multiple consulting engagements and enterprise implementations — I've sat in the rooms where enrollment automation gets proposed, scoped, deprioritized, and eventually re-proposed three years later. This time it's different. Here's why.
ACT I — 2018: THE PATIENT JOURNEY NO ONE COULD SEE
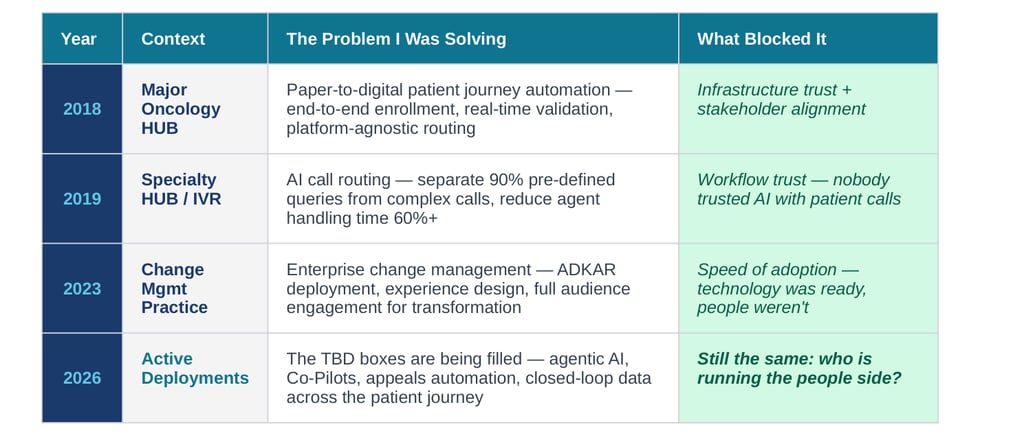
In 2018, I authored a patient journey automation proposal for a major oncology specialty distributor — a paper-to-digital transformation for one of the most complex HUB programs in the industry.
The patient journey we mapped had six stages: Referral & Diagnosis → Prescribe Drug → Reimbursement → Coordinate Care → Continued Care → Therapy Continuation. On paper, it looked like a clean handoff sequence. In practice, it was a series of gaps where patients fell through.
"How do we allow Providers to switch to using digital forms from paper forms, without introducing new variables and leveraging existing practice/provider infrastructure? Most importantly — the nut of the problem is validation. Easy as possible for the practice to start enrollment and get immediate f
And the governing principle for any solution — which I put at the top
Emphasis on Providers
Leverage existing infrastructure at practices
Minimal change to status quo for manufacturers
Platform Agnostic Solution (Plug and Play)
The technology to execute this didn't exist yet at scale. We delivered the architecture. We recommended the direction. We left a placeholder for the intelligent automation layer.
The placeholder said: TBD.
ACT II — 2019: THE 90% NOBODY WAS AUTOMATING
A year later, I built the business case for IVR Enhancement at a specialty pharma HUB.
We did a call analysis. What we found stopped the room.
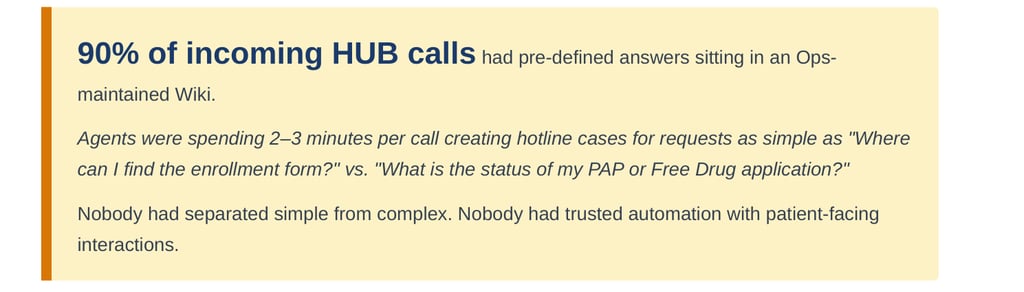
90% of incoming HUB calls had pre-defined answers sitting in an Ops-maintained Wiki.
Agents were spending 2–3 minutes per call creating hotline cases for requests as simple as "Where can I find the enrollment form?" vs. "What is the status of my PAP or Free Drug application?"
Nobody had separated simple from complex. Nobody had trusted automation with patient-facing interactions.
The Challenges/Risks section I wrote in that deck:
Time consuming. No identification of the nature of the call received by HUB agents — this results in hiring skilled personnel who should be prepared to answer any type of query, from simple to complex. Warm transfers may lead to additional hold time before talking to a human. Warm transfer may result in call drop-outs.
The dual objective I proposed:
We could not get buy-in to automate the patient-facing voice channel. It wasn't a technology problem. It was a trust and change management problem.
The TBD box stayed empty.
ACT III — 2023: THE CHANGE THAT COULDN'T BE BOUGHT
While leading change management engagements — including one that took me deep into the world of organizational effectiveness and transformation — the thread connecting every stalled initiative became impossible to ignore.
The methodology I was using was ADKAR — Awareness, Desire, Knowledge, Ability, Reinforcement. The framework for why people do or don't change.
The thesis at the heart of the practice:
" broad and deep capabilities focus on people and how they come together to bring vision and strategies to life. People are always essential to success."
I kept thinking about the 2018 patient journey map. The 2019 IVR proposal. The resistance hadn't been technical. It had been human:
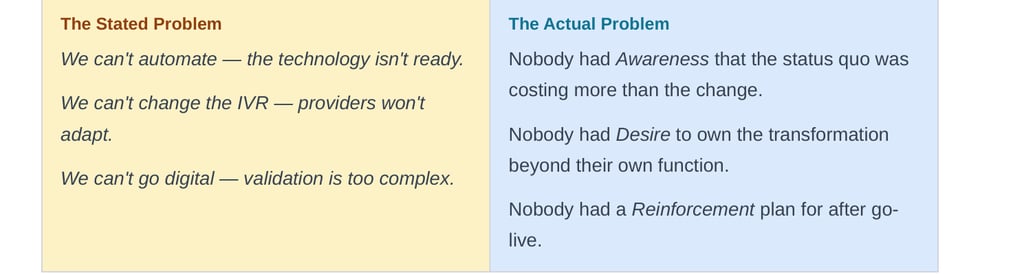
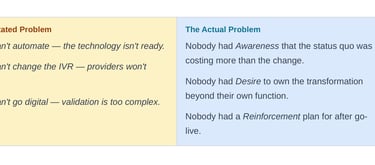
The Stated Problem
We can't automate — the technology isn't ready.
We can't change the IVR — providers won't adapt.
We can't go digital — validation is too complex.
The Actual Problem
Nobody had Awareness that the status quo was costing more than the change.
Nobody had Desire to own the transformation beyond their own function.
Nobody had a Reinforcement plan for after go-live.
ACT IV — 2026: THE TBD BOX IS FULL
The technology debate is over.
And a key forcing function accelerated everything: new state legislation has tripled pharmacy appeal volumes at some HUBs. What was once a manageable manual process is now operationally unsustainable. The business case that couldn't get funding in 2019 is now being approved in weeks.
In the last 18 months I have seen with my own eyes what teams are now executing:
Pharmacy appeals automation reading 50% of total appeal volume, auto-approving 50%+ of cases — $10-20M in recovered value, zero to production in under 60 days.
Agent Assist co-pilots replacing multi-system, multi-tab agent training with a single unified interface — the same outcome I proposed for IVR routing in 2019.
Clinical reporting co-pilots— saving approximately 2 hours per report per person. Ideas from whiteboard to production in weeks, not months.
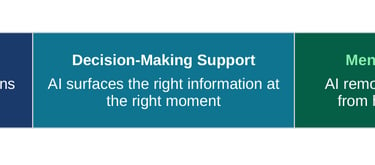
What these deployments share — beyond the ROI — is a design philosophy the industry is coalescing around. The HUBs that execute fastest aren't just picking the best AI stack. They are designing around three human-centric lenses:
The execution barrier is gone. Execution is no longer the bottleneck.
The next horizon is closer than most realize: AI-native products being architected directly into formulary and benefits management — not bolted onto legacy platforms, but built from the ground up around intelligent decision support. The window to shape how those products get deployed with people in mind is right now.
WHAT DIDN'T CHANGE
Everything I listed above is real. And every single one almost didn't happen — not because the AI wasn't ready, but because someone had to get the people ready first.
Look back at the governing principle I wrote in 2018:
Emphasis on Providers. Minimal change to status quo. Stakeholder view point — always.
I wrote that for a paper-to-digital migration in 2018. Read it again and tell me it isn't the governing principle for AI adoption in 2026.
The technology moved. The people dynamics didn't.
ADKAR is as relevant for AI as it was for replacing a fax machine. The HUBs that will win this transition aren't the ones who will buy the best AI stack — they're the ones who'll run the change program right alongside it.
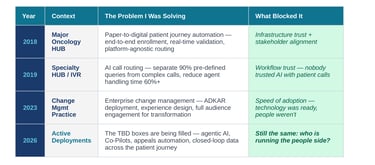
THE ARC — EIGHT YEARS, ONE CONSTANT
Year
Context
The
THE QUESTION FOR HUB LEADERS RIGHT NOW
You don't have a technology readiness problem. The platforms exist. The APIs are mandated. The business case is documented.
You have a PEOPLE READINESS PROBLEM.
And that's the one problem the AI cannot solve for itself.
If you are leading HUB operations, market access, or specialty pharma AI transformation and you want to talk about what the people side of this actually looks like in practice — I'd like to hear what you're navigating.
— Healthcare Transformation |
#SpecialtyPharma #HUBServices #AITransformation #ChangeManagement #HealthcareAI #PeopleFirst #PatientAccess